- Visibility 584 Views
- Downloads 57 Downloads
- Permissions
- DOI 10.18231/j.sajcrr.2023.023
-
CrossMark

Case report of palmoplantar psoriasis: Specific remedies to constitutional remedies for condition
Abstract
Introduction: Psoriasis, an autoimmune and chronic inflammatory disease of the skin, can leave the patient in agony with its distressing infection episodes. Palmoplantar psoriasis is a chronic variant of psoriasis that characteristically affects the skin of the palms and soles and produces significant functional disability. It features hyperkeratotic, pustular, or mixed morphologies. Palmoplantar psoriasis is a variant of psoriasis and accounts for 3–4% of total cases of psoriasis. Though historically difficult to treat, recent studies on biologic therapies have shown promising results for the treatment of palmoplantar psoriasis. This activity describes the pathophysiology, evaluation, and management of palmoplantar psoriasis and highlights the role of the interprofessional team in the care of affected patients. The homoeopathic system of medicine offers a wide range of medicines that can have a beneficial role in managing cases of psoriasis as depicted in the previous studies.
Objectives: 1. Identify the trigger factors and aetiology for palmoplantar psoriasis. 2. Describe the mental and physical presentation of a patient with palmoplantar psoriasis. 3. Summarize the out of treatment and management options available fin homeopathy for palmoplantar psoriasis. 3. Review interprofessional team strategies for improving care coordination and communication to enhance outcomes for patients affected by palmoplantar psoriasis. 4. Review of recurrence of palmoplantar psoriasis.
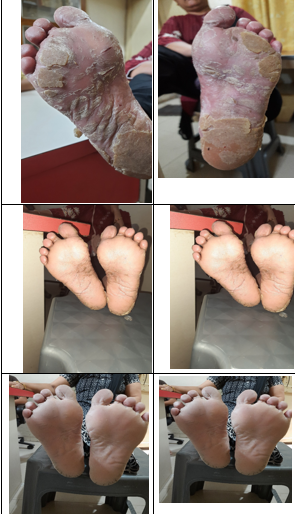
Case Summary: A distinct case of Palmoplantar psoriasis treated with homoeopathic remedies of ultrahigh potentised dilution has been presented here. The evidence-based illustrations were done before and after the treatment and the periodical objective assessment of the lesions with psoriasis area and severity index (PASI) calculation to ascertain the prognosis. The causal attribution of outcome to the treatment was evaluated using Modified Naranjo Criteria for Homoeopathy (MONARCH) tool. Marked improvement was found in the psoriatic lesions evidenced photographically and the PASI scores showed significant reduction affirming the same. The MONARCH score (+10) suggested that the clinical improvement was likely attributable to the homoeopathic treatment. This evidence-based case report suggests a beneficial role of homoeopathy in the treatment of palmoplantar psoriasis.
Introduction
Psoriasis is a common and chronic inflammatory condition of the skin, characterised by papulosquamous lesions with scaly and sharply demarcated red and indurated plaques, especially over extensor surfaces. It can appear anywhere on the skin, including the hands and feet. Palmoplantar psoriasis is a variant of psoriasis affecting the skin of the palms and soles with hyperkeratotic, pustular, or mixed presentations. Palmoplantar pustulosis or pustular palmoplantar psoriasis is characterised by small and sterile pustules. Both these chronic conditions produce significant functional disability and are associated with marked quality-of-life issues.
Demography of palmoplanter psoriasis
Even though the term palmoplantar psoriasis implies the involvement of both palms and soles, variability in the presentation does exist, with 59% of cases having both palmar and plantar lesions while exclusive palmar or plantar lesions are seen in 21% and 20% of patients, respectively. The palmoplantar variant of psoriasis is around 3–4% of all psoriasis cases, affecting 2–5% of the population.
Palmoplantar psoriasis affects individuals of all ages, while palmoplantar pustulosis is common between 20 and 60 years of age, with a clear female predominance.
Trigger factors and aetiology
Palmoplantar psoriasis is caused by a combination of genetic (HLA- B27) and environmental factors. Environmental triggers such as smoking, irritants, friction and manual or repetitive trauma augment the onset or aggravation of the lesion, pollutions, detergent, stress, hormonal imbalance person. It is common among farmers, homemakers and manual labourers with exacerbations from seasonal changes, an excess of household work, and exposure to detergents.
Appearance
Patients with palmer and plantar psoriasis report symptoms of well-defined areas of raised, thickened skin, scaling, itching, redness, burning sensation, pain, cracking with bleeding and small cracks. The patterns may be symmetrical. Palmoplantar psoriasis can significantly impact the quality of life with difficulty carrying out everyday activities such as walking and daily chores. The location of lesions makes it arduous to keep the lesions clean and hide them, leading to embarrassment and social anxiety.
Calculation score
PASI score is used for calculation and management of psoriasis. In this score, the severity (of three symptoms, erythema, induration and desquamation) and extent of involvement are calculated separately for four anatomical regions, namely, head, trunk, upper and lower limbs, as per their share in the total integument, on a 5-point scale from 0 to 4. The PASI score varies from 0 to 72. Higher scores indicate severer conditions. The score is also helpful for assessing prognosis during the treatment.
Treatment of recent era in modern medicine
Conventionally, first-line therapy begins with potent to super potent topical corticosteroids. However, most patients require systemic agents given the obstinate nature of these skin diseases. According to the American Academy of Dermatology, some systemic medications for psoriasis include methotrexate, cyclosporine and apremilast; all are effective but with their contraindications and side effects. Common side effects of topical treatments include irritation, skin thinning and skin dryness; oral therapies include gastrointestinal problems and interactions with other drugs. Considering the multi-factorial causation, chronicity of complaints and kaleidoscopic presentation of psoriasis, homoeopathy, with its holistic and individualistic approach, can be an effective alternative in the treatment of psoriasis.[1], [2], [3], [4], [5]
Approach of homeopathy
In a prospective, multicentric and observational study to evaluate details and effects of homoeopathic treatment in patients with psoriasis in usual medical care, the diagnoses and complaints severity improved markedly with large effect sizes along with improvement in quality of life, while conventional treatment and health service use were considerably reduced. In a study ‘Evaluation of Homoeopathic drugs in psoriasis’, numbers of cases were evaluated and a group of homoeopathic remedies such as Arsenicum album, Hydrocotyleasciatica, Ignatia amara, Tuberculinum, Calcareacarbonica, Kali arsenicosum, Lycopodium clavatum, Natrum muriaticum, Nux vomica, Opium, Petroleum, Psorinum, Sepia, Sulphur and Thyroidinum were found to be effective in the treatment of psoriasis. One of specific remedy is indicate in boeriekmateria medica is Corralium Rubrum. In repertory of homeopathy, total 31 medicines are indicated in psoriasis on palm and total 12 medicine are in psoriasis on sole – both rubrics covered by few medicines like arsenicum album, Arsenicumiodatum, Graphites, Corallium, Kali Arsenicum, Kalium Sulphuricum, Mercurius, Petroleum, Phosphorus. Selenium, Sepia Given the chronic nature of the disease and the need for prolonged treatment, complementary and alternative medicine use has become common in psoriasis. In this context, the present case report, presenting a severe form of palmoplantar psoriasis managed with individualised homoeopathic medicines, emphasises the positive role of homoeopathy, one of the most popular alternative therapies in the management of psoriasis.
|
No. |
Modified Naranjo’s Criteria Algorithm |
Yes |
No |
Not sure or N/A. |
|
1 |
Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? |
2 |
|
|
|
2 |
Did the clinical improvement occur within a plausible timeframe relative to the medicine intake? |
2 |
|
|
|
3 |
Was there a homeopathic aggravation of symptoms? |
|
0 |
0 |
|
4 |
Did the effect encompass more than the main symptom or condition (i.e., were other symptoms, not related to the main presenting complaint, ultimately improved or changed)? |
|
|
|
|
5 |
Did overall well-being improve? |
2 |
|
|
|
6 |
(A) Direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? (B) Direction of cure: Did at least one of the following aspects apply to the order of improvement of symptoms: - From organs of more importance to those of less importance? - From deeper to more superficial aspects of the individual? - From the top downwards? |
- |
- |
0 |
|
7 |
Did ‘old symptoms’ (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? |
- |
|
0 |
|
8 |
Are there alternative causes (i.e., other than the medicine) that –with a high probability – could have produced caused the improvement? (Consider known course of disease, other forms of treatment and other clinically relevant interventions) |
- |
0 |
- |
|
9 |
Was the health improvement confirmed by any objective evidence? (e.g., investigations, clinical examination, etc.) |
2 |
- |
- |
|
10 |
Did repeat dosing, if conducted, create similar clinical improvement? |
2 |
- |
- |
|
Date |
Symptoms |
Prescription |
|
16/05/2022 |
|
Corallium 30/OD Sac.Lac BD External Application-Petroleum Q and coconut oil. For 7 days |
|
22/05/2022 |
Cracks are present Redness slightly decreases. |
Corallium 30/OD Sac. Lac BD External Application as it is |
|
29/06/2022 |
During treatment small cracks appeared on hand |
Corallium 200/OD Sac.Lac BD External Application only coconut oil |
|
5/06/2022 |
No such improvement |
Medicine as it is |
|
19/06/2022 |
Cracks and burning increase |
Lachesis 30/BD Sac. Lac OD External Application – Coconut Oil Medicine for 15 days |
|
3/07/2022 |
No new symptoms. Redness decrease |
Same medicine for 15 days |
|
17/07/2022 |
Decrease redness, cracks start to heal. Burning decrease |
Same medicine for 15 days |
|
31/07/2022 |
Decrease complaints |
Same medicine for 15 days |
|
14/08/2022 |
Decrease complaints |
Same medicine for 15 days |
|
28/08/2022 |
Decrease complaints |
Same medicine for 15 days |
|
1/09/2022 |
Decrease complaints |
Same medicine for 15 days |
|
18/09/2022 |
Few new cracks appeared. Due to some hot weather |
Merc. Sol -30 for 15 days. With external application of coconut oil |
|
1/10/2022 |
Complaints decrease |
Merc sol -30 for 15 days. With external application of coconut oil |
|
15/10/2022 |
Decrease complaints. |
Lachesis 200- BD For 15 days. With external application of coconut oil |
|
30/10/2022 |
Decrease complaints |
Sac.Lac for 1 month |
|
30/11/2022 |
No any complaints |
Sac.Lac for 1 month |
|
31/12/2022 |
No any complaints |
Sac.Lac for 1 month |
|
28/01/2023 |
No any complaints |
Sac. Lac for 1 month |
|
28/02/2023 |
No complaints |
Sac.Lac bd for 1 month |
|
28/03/2023 |
Slightly -Burning and redness and itching appeared |
Lachesis- 200/1 dose Sac .Lac for 1 month |
|
28/04/2023 |
No any complaints |
Sac. Lac for 1 month |
|
28/05/2023 |
No any complaints |
Sac. Lac for 1 month |
|
22/06/2023 |
No any complaints |
Sac.Lac for 1 month |
|
26/07/2023 |
No complaint |
No medicine |

Materials and Methods
Sample- Selective Case study
Study- Analytic study Method
Comparative before and after study.
Study Place- Yogeshwar Homoeopathic Clinic, Surat
Tool- Monarch Score And PASI Score tool, Homeopathic software (Zomeo), Homeopathic Materia Medica.
Procedure -Before start treatment, verbal consent and written consent given by patient for her treatment. After our team use two score for psoriasis evolution and take photo of psoriatic lesions which are present on body part. Follow up of patient is every 15 days. Every follow up, our team take photo of psoriasis for comparison. After treatment evaluate by MONARCH testand PASI tool for comparison of psoriasis.[6], [7], [8], [9]
Patient information
A female aged 54 years with a history of cracks on soles for many years, with scaling, itching and bleeding; presented with acute exacerbation of the psoriasis. The present complaints had occurred after 15 weeks with burning and redness in sole and palm. There was severe burning pain and hot feeling in the lesions with hard yellowish skin. Recurrent cracks develop on palm and sole, which burning on touching the water. Other associated symptoms included a burning on tongue particular left side of edge with clean and pointed tongue and centrally crack on tongue, salivation profuse during sleep. There was difficulty with an inability to cope with her daily house hold routine. Based on the presentation, the patient was given increasing potencies of Corallium from 30 to 200 and his lesions healed in 8 weeks. [10], [11], [12], [13], [14]
Later, during the subsequent visit
There was the intensity of symptoms were constantly changing. There was dryness, scaling, cracks and thickness skin in both palm and sole decrease but burning and hot feeling were not decreases. After her tour, symptoms were reappeared which were decreases. The patient had history of scanty menses at 13 years of age. She was taken medicine for few months but not too much recovery. Her mother was died due to suffering from blood cancer and her father was suffer from joint pain. She conceived pregnancy with at age of 20 and child born with normal delivery. Her appetite was good. Her thirst was like thirstlessness because whole day she took only 2-3 glasses per 24 hours. Her bowels were regular, urine dark yellow. Her sleep was disturbing due to her granddaughter many times awake in between sleep. She desires spicy and salty food. She least like to take milk. Patient was talkative, communicative by nature. Every time she ask one question.’ ‘Doctor, this disease could be cured by homeopathy? Second presentation - “I had taken three-month medicine but only partial relief, how much time you will take for my recovery? Third presentation – shall I pay money after recovery? Fourth presentation - every time take full charges, please give some concession
Clinical findings He was mesomorphic with a fair complexion. His pulse rate was 62/min; his heart rate was 76/min; temperature was 98.6°F and his blood pressure was 126/88 mm of Hg. Locally, there were cracked lesions with thickened skin on the soles of both feet, with. There were cracks with minute bleeding on the lateral and back aspect of the both feet. Right foot toe slightly thick. At baseline, the PASI score was 28.6. Based on the history and clinical findings, he was diagnosed to have plantar psoriasis (ICD 10 classification code L40.3).[15], [16], [17], [18], [19], [20]
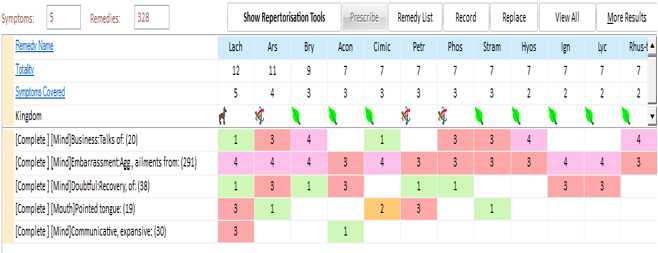
The totality of symptoms taken for repertorisation was
Business talk, talkativeness, communicative expansive, doubtful of recovery. burning sole and palm, burning left edge of tongue, pointed tongue. Clean tongue. Cracks on middle of tongue. Menses scanty with three days. Summer season psoriasis problem increase.[21], [22]
Based on repertorization – mental and physical general symptoms were covering the Lachesis medicine. Lachesis medicine prescribed on gradually increasing potency. Acute exacerbations during the follow-up period were prescribed as per the acute totality. Maintenance of general hygiene of the area and avoidance of walking on bare feet decrease use of divergent during washing of cloth were advised to the patient.
Follow-up and outcome
In the initial visit, the patient presented with a decrease of psoriatic patches on the palm and sole. After few months later, begging of summer, her palm become rougher and more cracked with burning. Based on the acute totality, the patient was given increasing potencies of Mercurius solubilis from 30 and her lesions improved in 2 weeks. Later, during the subsequent visit, a detailed case history was taken and based on the analysis and repertorisation of the available totality, the remedy Lachesis was selected. The case was followed up for 1 year. During the follow-up, Lachesis 200 was continued for 1 year. After Lachesis, there was gradual but constant improvement in the patient’s symptoms and general well-being. The objective assessment scale of the local lesions, PASI, was applied to the case periodically at 1-year intervals, and a substantial reduction in the score, from the baseline score of 28.6–1.3, was noted by the end of the follow-ups. The Modified Naranjo Criteria are applied to this case for ascertaining the causal attribution between the homoeopathic medicine applied and the changes in the symptoms/signs of the patient.
Discussion The case report describes the utility of homoeopathic treatment in the management of psoriasis. This case of plantar psoriasis with severe symptoms has improved with individualised homoeopathic treatment. Merc sol and Corallium, the remedy selected initially, based on the acute totality and therapeutic, is known for its action in psoriasis affections. With repetition, in increasing potency, it relieved the initial troublesome symptoms of the patient. However, considering the frequent recurrence of the complaints, at a subsequent visit, the remedy Lachesis was given based on analysis of the constitutional totality, repertorisation and consultation with Materia medica. The symptoms of acute exacerbations could not be included in repertorisation because the presentation was only limited to the period of exacerbation. Hence, Merc sol did not come up in repertorisation. Initially, the remedy Lachesis was given in 30th potency with mild effective on psoriasis. Later, the same was given in the next higher potency, 200.
Considering the symptomatology and pathology, the case appeared to be Psoro-syco-syphilitic. During the acute exacerbations, the symptoms pertaining to syphilitic miasm appeared to be dominant and accordingly, the more troublesome symptoms of initial presentation responded well to Mercurius solubilis. Later, the totality of symptoms, together with the thickened skin, represented Psoro-sycotic predominance and the remedy Lachesis was selected based on symptom similarity with marked improvement in the complaints.
Condition of the patient
The frequency of acute exacerbations of the foot lesions gradually decreased. Improvement in the local lesions is evident from the substantial reduction in the PASI score from the baseline value of 28.6–1.3 by the end of the follow-up. As per the modified Naranjo Criteria, there was an improvement in the primary symptom (+2); within a plausible timeframe after the intake of medicine (+2); with an improvement in other symptoms (+2) and overall well-being (+2); with no other alternative causes that could have caused the improvement (+2). Further, there was an objective improvement in the skin lesions after the remedy, evidenced by photographs and PASI score (+2). The remedy, on repetition of dose, has resulted in a similar clinical improvement (+2). Thus, in this case, the total score of 10 establishes a definite causal attribution of homoeopathic treatment with the outcome.
Conclusion
In this case, the individualised homoeopathic treatment helped in healing of acute exacerbation and chronic lesions of psoriasis on the palm and sole, together with gradual improvement in general well-being with no recurrence of psoriasis after completing the treatment. this case hints at the positive role of homoeopathy in the treatment of psoriasis and other auto immune diseases.
Source of Funding
None.
Conflict of Interest
None.
Acknowledgment
In performing case study, I had to take the help and guideline of some respected person and scientific team person who deserved my greatest gratitude. First, I would like to show my gratitude to Mr, Kevin Kumar (Occupational Health Officer) and CCRH team,
References
- Asumalahti K, Ameen M, Suomela S, Hagforsen E, Michaëlsson G, Evans J. Genetic analysis of PSORS1 distinguishes guttate psoriasis and palmoplantar pustulosis. J Invest Dermatol. 2003;120(4):627-59. [Google Scholar]
- Barrea L, Savanelli M, Somma D, Napolitano C, Megna M, Colao M. Vitamin D and its role in psoriasis: An overview of the dermatologist and nutritionist. Rev Endocr Metab Disord. 2017;18(2):195-205. [Google Scholar]
- Boericke W. . New Manual of Homoeopathic Materia Medica and Repertory. 2000. [Google Scholar]
- Cotosegura P, Fernandez D, Batalla A, Gomez J, Gonzalezlara L, Queiro R. Common and rare CARD14 gene variants affect the antitumour necrosis factor response among patients with psoriasis. Br J Dermatol. 2016;175(1):134-75. [Google Scholar]
- Farley E, Masrour S, Mckey J, Menter A. Palmoplantar psoriasis: A phenotypical and clinical review with introduction of a new qualityof-life assessment tool. J Am Acad Dermatol. 2009;60(6):1024-55. [Google Scholar]
- Gupta G, Gupta N, Pandey D. Psoriasis: Best case series. Homeopathic Links. 2019;32(2):64-76. [Google Scholar]
- Hering C. The Guiding Symptoms of our Materia Medica. . 1984. [Google Scholar]
- Huizen J. Palmoplantar psoriasis: What you need to know. . 2018. [Google Scholar]
- Huzar T. Psoriasis Oral Medications: List and Side Effects. . 2018. [Google Scholar]
- Kanwar A, Ram H, Kumar N, Bagdi N. Plaque psoriasis successfully treated with an individualised homoeopathic medicine Lycopodium: A case report. . . [Google Scholar] [Crossref]
- Khandpur S, Singhal V, Sharma V. Palmoplantar involvement in psoriasis: Aclinical study. Indian J Dermatol Venereol Leprol. 2011;77(5). [Google Scholar] [Crossref]
- Kingo K, Mossner R, Koks S, Ratsep R, Kruger U, Vasar E. Association analysis of IL19, IL20 and IL24 genes in palmoplantar pustulosis. Br J Dermatol. 2007;156(4):646-52. [Google Scholar]
- Lamba C, Gupta V, Haselen R, Rutten L, Mahajan N, Molla A. Evaluation of the modified Naranjo criteria for assessing causal attribution of clinical outcome to homeopathic intervention as presented in case reports. Homeopathy. 2020;109(4):191-8. [Google Scholar]
- Miceli A, Schmieder G, Psoriasis P. . Treasure Island (FL): Stat Pearls Publishing. ;2022. [Google Scholar]
- Obregon A. Psoriasis as a systemic disease. Clin Dermatol. 2012;32(3):159-216. [Google Scholar]
- Ortega P. . Notes on the Miasms or Hahnemann’s Chronic Diseases. New Delhi: National Homoeopathic Pharmacy. 1980. [Google Scholar]
- Rahman S, Dey J. A case report of plantar psoriasis treated with homoeopathy. Homeopathic Links. 2018;31(4):248-53. [Google Scholar]
- Schmitt J, Wozel G. The psoriasis area and severity index is the adequate criterion to define severity in chronic plaque-type psoriasis. Dermatology. 2005;210:194-203. [Google Scholar]
- Singh H, Manchanda R, Arora S. Evaluation of homoeopathic drugs in psoriasis. CCRH Quarter Bull. 1990;12:22-30. [Google Scholar]
- Talbott W, Duffy N. Complementary and alternative medicine for psoriasis: What the dermatologist needs to know. Am J Clin Dermatol. 2015;16(3):147-65. [Google Scholar]
- Timotijevic Z, Trajkovic G, Jankovic J, Relic M, Doric D, Vukicevic D. How frequently does palmoplantar psoriasis affect the palms and/ or soles? A systematic review and meta-analysis. Postepy Dermatol Alergol. 2019;36(5):595-603. [Google Scholar]
- Witt C, Lüdtke R, Willich S. Homeopathic treatment of patients with psoriasis--a prospective observational study with 2 years followup. J Eur Acad Dermatol Venereol. 2009;23(5):538-81. [Google Scholar]
- Abstract
- Introduction
- Demography of palmoplanter psoriasis
- Trigger factors and aetiology
- Appearance
- Calculation score
- Treatment of recent era in modern medicine
- Approach of homeopathy
- Materials and Methods
- Comparative before and after study.
- Patient information
- Later, during the subsequent visit
- The totality of symptoms taken for repertorisation was
- Follow-up and outcome
- Condition of the patient
- Conclusion
- Source of Funding
- Conflict of Interest
- Acknowledgment
- References