

Introduction
Histoplasma capsulatum is a thermal dimorphic fungus. Human infection by H. capsulatum, histoplasmosis has a broad spectrum of clinical manifestations ranging from a self-limited, acute influenza-like illness to a progressive disseminated infection that is life threatening. Though histoplasmosis is an acquired immunodeficiency syndrome (AIDS) defining illness, oral involvement is rare as its initial manifestation.
Case Report
A 23-year-old female homemaker presented with painful oral ulcer and painful swallowing of 3 months duration. Oral ulceration involved the roof of mouth, tongue and lower lip. The ulcerated area was covered by membranous exudate and pus. She also had reduced appetite and significant weight loss (15% from baseline over 3 months). Significant negative history included absence of fever, genital ulcers, rash, arthralgia, nasal regurgitation, anesthetic skin patches, claudication pain, cough, hemoptysis, nosebleeds, nasal discharge, collapse of nasal bridge, hearing loss, high colored urine, reduced urine output, or trauma to oral cavity. She had no history of any chronic illnesses. She gave no history of intravenous drug abuse. Patient had been married for 6 months prior to presentation and was in a monogamous relationship with her husband. She denied any prior high-risk sexual behavior. Physical examination revealed bilateral multiple 2 x 2 cm firm, tender, non-matted level Ib, II, III cervical lymphadenopathy. There was an extensive oral ulcer involving uvula, soft palate and hard palate. The borders of the ulcer were edematous and raised, the floor appeared granular, and was covered with slough (Figure 1). The ulcer was tender and non-indurated on palpation. Two perforations were also noticed in the hard and soft palates (Figure 2). Tongue was covered with a membrane which could be scraped off easily (Figure 3). Other systemic examinations were unremarkable.



Figure 4
FNAC lymphnode showing small round budding narrow based yeast cells inside macrophage suggestive of Histoplasma capsulatum.

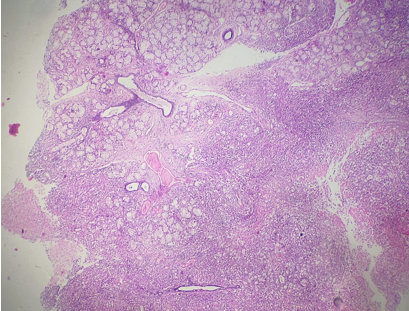
Figure 6
Palatal biopsy shows small round budding narrow based yeast cells inside macrophage suggestive of Histoplasma capsulatum


Complete blood count with differential count revealed normocytic anemia (hemoglobin 8.1 g/dL), normal total white blood cell count (8.5 x109/L) and mild thrombocytosis (475 x109/L), and raised erythrocyte sedimentation rate (105 mm in 1 hour). Metabolic panel showed hypoalbuminemia (3g/dL). Liver function tests and renal function tests were normal. Anti-nuclear antibody (ANA) by immunofluorescence was negative. Contrast enhanced computed tomography scan of chest and abdomen were unrevealing. Patient tested positive for human immunodeficiency virus (HIV) type 1 infection using enzyme linked immunosorbent assay (ELISA) and this was confirmed using western blot assay. CD4+ T-lymphocyte count was below the threshold for detection in our laboratory. A fine needle aspiration from the cervical lymph node and a palatal biopsy revealed small budding narrow based yeast cells inside macrophages suggestive of H. capsulatum (Figure 4, Figure 5, Figure 6, Figure 7). On further exploration it was revealed that both her parents were HIV positive receiving antiretroviral therapy for past 7 years, suggesting likely vertical transmission to the patient. However, the history of parental infection was concealed so far. Patient was treated for histoplasmosis with injection liposomal amphotericin B 3mg/kg intravenously and itraconazole 200mg orally for 1 year. She was also initiated on highly active antiretroviral therapy (HAART) with daily oral tenofovir, lamivudine and dolutegravir. One year after initiation of HAART her CD4+ T-cell count increased to 354 cells/µL and viral load was undetectable. Her oral ulcers healed well and a palatal prosthesis was placed for the palatal perforations.
Discussion
Histoplasmosis is a systemic fungal infection caused by H. capsulatum, usually seen in immunocompromised individuals such as those with HIV-AIDS. The microconidia in the soil are the infective forms. The important risk factors for histoplasmosis are CD4+ T-cell count below 150/µL, exposure to chicken coops and prior exposure to H. capsulatum as evidenced by sensitivity testing.1 The lungs are the primary location of infection, from which it can spread to any other organ. In immunocompetent persons, infection is usually self-limited with influenza like symptoms; calcified lung nodules, mediastinal lymph nodes and hepatosplenic calcification may be incidentally found in healthy individuals of endemic regions.2 The clinical features may range from self-limited pulmonary manifestations to disseminated multiorgan involvement. Oral lesions as the first and only sign of AIDS is indeed rare.3, 4, 5 The tongue, hard and soft palate, buccal mucosa, gingiva, and lips are the most often affected areas in the oral cavity.3, 6, 7, 8 Oral lesions can appear as papules, ulcers, nodules, vegetative, granulomatous, or plaque-like lesions. A superficial or deep infiltrating ulceration with a pseudo membrane is the most typical presentation.3, 6, 7, 8 Palatal perforation secondary to histoplasmosis has been reported only rarely.9, 10, 11
Though common in North, central and south American countries, in India the Gangetic basin is endemic for histoplasma capsulatum. 12 Most cases have been reported from West Bengal, Rajasthan, Maharashtra, Haryana and Bihar.12 Reports of histoplasmosis from Kerala are limited. Five cases reported from Kottayam district of Kerala presented as fever or generalised lymphadenopathy. A case from Kozhikode district in Kerala also presented with cervical lymphadenopathy. There are anecdotal reports of histoplasmosis presenting as a nodulo-ulcerative growth on the hard palate from Kerala.2 To the best of our knowledge palatal perforation as the initial presentation has not been reported previously from South India.
Histopathological examination of involved tissue and fungal culture are the gold standard tests for diagnosis. On direct microscopic examination of smears from clinical specimens, yeast cells are seen as small, ovoid 2-5 micron sized structures, with a single bud attached by a narrow base, seen extracellularly or within macrophages.13 The urine and serum antigen testing have high sensitivity and specificity in disseminated histoplasmosis.14 Progressive disseminated histoplasmosis is treated initially with intravenous lipid formulation Amphotericin B (3-5 mg/kg/day) or conventional Amphotericin B (0.7-1 mg/kg/day) for 1-2 weeks; then oral itraconazole (200 mg twice daily) should be continued for 12 months.15 Immune reconstitution inflammatory syndrome associated with histoplasmosis is unusual, occurring at about 0.74 cases per 1,000 person-years among people living with HIV.15 Some experts suggest prophylaxis with itraconazole at a dose of 200 mg daily to patients with CD4 counts <150 cells/mm3 who are at high risk because of occupational exposure or who live in a community with a hyperendemic rate of histoplasmosis (>10 cases/100 patient-years).16
Conclusion
HIV-AIDS could manifest for the first time as a potentially fatal opportunistic infection like histoplasmosis. Though oral manifestations are rare, they could be the only presenting symptom of disseminated histoplasmosis. Differentials like histoplasmosis should be considered in cases of unusual exaggerated oral ulcerations. A high index of suspicion is needed in such cases, as delay in diagnosis and therapy can lead to multiorgan failure and death.